
The Monthly Board Meeting: What Ovulation Can Reveal About Hormone Resilience, Metabolic Chaos® & Midlife
The Monthly Board Meeting: What Ovulation Can Reveal About Hormone Resilience, Metabolic Chaos® & Midlife
🌺 Ladies, Your Ovaries Have Been in the Meeting All Along
Let’s have a grown-woman conversation.
For years, many of us were taught to think about ovulation through one narrow lens:
Can I get pregnant?
Trying for a baby? Track it.
Avoiding pregnancy? Prevent it.
Finished having children—or never wanted them?
Apparently, ovulation was no longer your concern.
Except female physiology is far more interesting than that.
Ovulation is a reproductive event, yes. But it is also part of a much larger endocrine conversation involving your brain, pituitary gland, ovaries, oestradiol, progesterone and multiple feedback loops.
After ovulation, the ruptured follicle becomes the corpus luteum, which produces the major cyclical rise in progesterone during the luteal phase.
That matters whether you want:
👶🏾 a baby
🚫 absolutely no baby
💼 a boardroom
📖 ministry
🏋🏾♀️ stronger muscles
🌍 more stamps in your passport
😴 or simply one decent night of sleep without waking at 3:07 a.m. with seventeen thoughts and a grocery list
Ovulation is not your entire health story.
But it can be an important chapter.
So perhaps the better question is not simply:
“What supplement should I take?”
Perhaps it is:
“What is this pattern trying to tell us?”
Now we are getting somewhere. 🌿
🧠 Ovulation Actually Begins in the Brain
Yes, the ovaries get all the publicity, but the brain is very much involved.
Your menstrual cycle is coordinated through the hypothalamic-pituitary-ovarian axis, or HPO axis.
In simple terms:
Hypothalamus → GnRH → Pituitary → FSH and LH → Ovaries → Oestradiol → Ovulation → Progesterone
Here is the monthly board meeting:
🌱 FSH supports follicular development
🌹 Oestradiol rises as the follicle develops
⚡ An LH surge helps trigger ovulation
🌙 The ruptured follicle becomes the corpus luteum
💛 Progesterone rises after ovulation
So no, ovulation is not simply:
“Did an egg come out?”
Technically important?
Yes.
The whole story?
Not even close.
Ovulation tells us something about communication between the brain and ovaries. It is part of a coordinated endocrine event—not merely a fertility switch.
🌙 The Progesterone Plot Twist
Progesterone is one of the most misunderstood hormones in women’s health.
And before the hormone wars begin, let me say this clearly:
I am not interested in making progesterone the angel and oestrogen the villain.
That social-media nonsense needs to retire.
Oestrogen matters.
Progesterone matters.
Androgens matter.
Thyroid hormones matter.
Insulin matters.
Cortisol matters.
The pattern matters. The woman matters.
After ovulation, the corpus luteum becomes the major source of the normal cyclical rise in progesterone.
So I would not say:
“Without ovulation, the body makes literally zero progesterone.”
That is too absolute.
But I would say:
Without ovulation, you do not get the normal corpus-luteum-driven post-ovulatory progesterone rise.
And that is a meaningful endocrine difference.
Progesterone biology also extends beyond pregnancy. Progesterone-derived neurosteroids interact with the nervous system, including GABA-A receptor pathways, which is one reason progesterone is studied in relation to sleep, mood and neurological function.
But no, I am not going to tell every anxious woman:
“You just need progesterone.”
One woman may benefit from appropriately prescribed micronised progesterone.
Another may have iron deficiency.
Another may have thyroid dysfunction.
Another may be under-fuelling.
Another may have a PMOS-type pattern.
Another may be moving through perimenopause.
And another may have several things happening at once.
Welcome to what I call:
Metabolic Chaos®
Because bodies are not spreadsheets, and women are not identical lab rats wearing matching cardigans. 😌
🌹 Oestrogen Is Not the Villain Either
Oestradiol plays an important role in follicular development and the hormonal events leading toward ovulation.
Oestrogen signalling also matters across tissues including:
🦴 bone
🧠 brain
🌸 reproductive tissues
💧 genitourinary tissues
🩸 blood vessels
But hormones are not simply “good” or “bad.”
Their effects depend on context:
age
reproductive stage
timing
dose
route
medical history
underlying risk
individual response
That is why I refuse to reduce women’s hormones to bumper stickers.
The better question is:
What is the pattern, what is the context, and what is happening in this particular woman?
That is grown-woman science.
🩸 A Period Does Not Automatically Prove Ovulation
This surprises many women.
You can bleed without completing a typical ovulatory cycle.
So:
Monthly bleeding does not automatically prove monthly ovulation.
That is why I ask more than:
“When was your last period?”
I want to know:
Are your cycles becoming shorter?
Longer?
More variable?
Are you spotting?
Bleeding heavily?
Passing larger clots?
Has your sleep changed?
Anxiety?
Migraines?
Libido?
Training load?
Food intake?
Iron status?
Thyroid history?
Because a period tracker gives me dates.
I am interested in the story.
And sometimes the story is showing us that the cycle is changing before the woman fully realises it.
⚡ When Ovulation Goes Offline, We Need to Ask Why
Persistent anovulation is not one disease.
Potential contributors may include:
pregnancy
PMOS
thyroid dysfunction
elevated prolactin
low energy availability
significant psychological stress
eating disorders
excessive exercise relative to fuelling
primary ovarian insufficiency
medication effects
perimenopause
other endocrine or structural conditions
This is why I become twitchy when every woman with cycle disruption is told:
“It’s just stress.”
Could stress matter?
Absolutely.
But could it be thyroid dysfunction?
Yes.
PMOS?
Yes.
Perimenopause?
Yes.
Pregnancy?
Also yes.
So we investigate.
Because “just balance your hormones” is not a diagnosis.
Fun Fact Science Bar+ Your Ovulation May Leave a Thermal Fingerprint 🌡️🌙
🔬 Fun Fact Science Bar+ Your Ovulation May Leave a Thermal Fingerprint 🌡️🌙
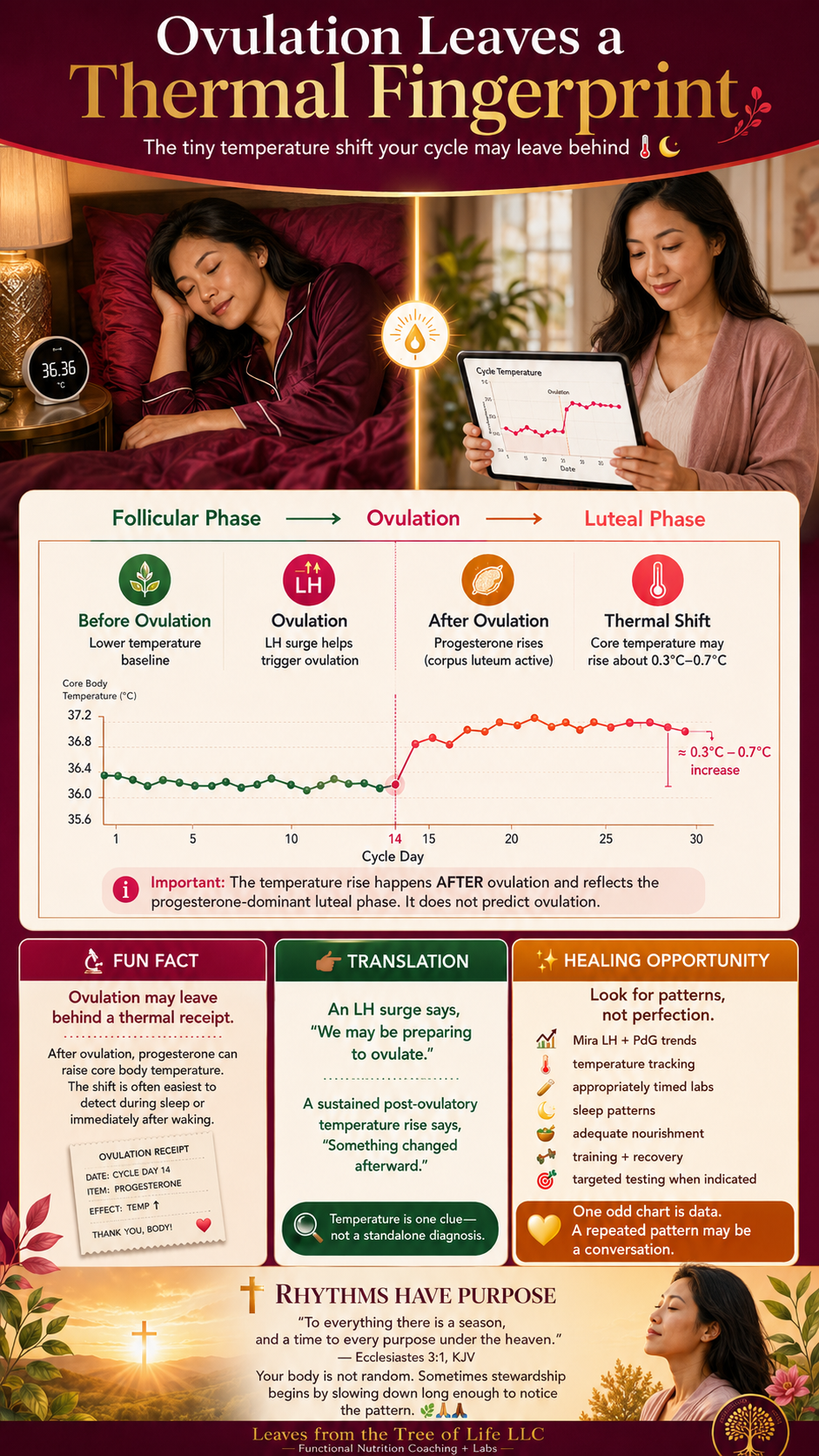
Did you know that after ovulation, rising progesterone can increase core body temperature by roughly 0.3°C to 0.7°C during the luteal phase? This shift is often easiest to spot during sleep or first thing in the morning—before coffee, exercise, or grown-woman chaos begins. 😅
👉🏾 Translation: Ovulation may leave behind a small thermal receipt. 🧾🌡️ An LH surge suggests the body is preparing to ovulate, while a sustained temperature rise afterward can offer another clue that the cycle moved into a progesterone-influenced luteal phase. Useful? Yes. A standalone diagnosis? No ma’am.
✨ Healing Opportunity: If your usual temperature pattern becomes erratic or disappears alongside irregular cycles, poor sleep, under-fuelling, heavy training, thyroid concerns, PMOS-type patterns, or perimenopause, look at the wider story. Track trends over time, pair them with symptoms and tools such as Mira LH and PdG patterns, and investigate persistent changes appropriately.
One odd chart is data. A repeated pattern may be a conversation.
✝️ Faith Element: God designed the body with rhythms—light and darkness, activity and rest, seasons and transitions.
“To every thing there is a season, and a time to every purpose under the heaven.” — Ecclesiastes 3:1, KJV
Sometimes stewardship begins by slowing down long enough to notice the pattern. 🌿🙏🏾
🍽️ Some High-Achieving Women Are Simply Not Eating Enough
Let me lovingly step on a few toes.
Some women are trying to run:
💼 a company
🏡 a household
📚 a ministry
🏋🏾♀️ a training programme
✈️ international travel
on:
☕ coffee
🥬 half a salad
🥜 seven almonds
😵💫 anxiety
🙏🏾 one Bible verse
and sheer determination
Ma’am. We need lunch.
Low energy availability can disrupt reproductive signalling in susceptible women, especially when inadequate intake is combined with high training demand, weight loss or significant stress.
And no, a woman does not have to “look underweight” before this becomes relevant.
She may be eating beautifully and still not be eating enough.
Those are not the same thing.
Sometimes the healing opportunity is not another cleanse.
It is nourishment.
🎢 Perimenopause: When the Monthly Board Meeting Gets Rowdy
Now to my midlife ladies.
You may have had predictable cycles for decades.
Then suddenly:
24 days.
37 days.
Skipped month.
Heavy bleeding.
Barely any bleeding.
Insomnia.
Anxiety.
Migraines.
Bloating.
Brain fog.
…and one random glorious month where you feel completely normal before the hormonal circus returns with snacks. 🎪
Perimenopause involves changing ovarian function, and ovulation may become less predictable.
That does not mean your body has suddenly become incompetent.
It means you are entering a different reproductive season.
And this is where testing requires wisdom.
I believe in:
Test, don’t guess.
But I also believe:
Do not test without a question.
A pile of expensive laboratory reports is not personalised care.
🧩 Metabolic Chaos®: The Symptoms May Be Connected
A woman may experience:
😰 anxiety
🎈 bloating
🩸 heavy periods
😴 poor sleep
📉 low energy
🎢 irregular cycles
🧠 brain fog
Each symptom may be treated as a separate problem.
But sometimes I see a network.
For example:
Heavy bleeding → iron depletion → exhaustion → poorer recovery
Restrictive eating → inadequate energy availability → disrupted reproductive signalling
Poor sleep → fatigue → more caffeine → worse sleep
GI symptoms → increasing food restriction → lower nutrient intake → poorer resilience
That interconnected pattern is what I mean by:
Metabolic Chaos®
It does not mean your body is stupid.
It means several systems may be interacting.
And where others see chaos?
I start looking for healing opportunities.
🌿 Supporting Ovulation: Start With the Driver
Natural support should be matched to the woman and the reason ovulation is changing.
A woman with low energy availability is not the same as:
a woman in late perimenopause
a woman with PMOS
a woman with primary ovarian insufficiency
a woman with thyroid dysfunction
a woman using hormonal contraception
Different pattern.
Different tools.
Different conversation.
🥑 Nourish Before You “Hack”
For a whole-food plant-based woman, supportive nutrition may include:
🫘 beans and lentils
🌱 tofu and tempeh
🥑 avocado
🥜 nuts and seeds
🌾 intact whole grains
🍠 root vegetables
🫐 berries
🥦 colourful vegetables
But I am also asking:
Are you eating enough?
Enough protein?
Enough carbohydrate for your activity level?
Adequate dietary fat?
Are you skipping meals and calling it hormone support?
Because sometimes the healing opportunity is not another cleanse.
It is lunch.
💊 Supplements & Nutraceuticals: Match the Tool to the Pattern
Supplements are tools.
Not tiny edible miracles.
Depending on the actual pattern, a practitioner may consider:
🌞 vitamin D
🩸 iron when indicated
🌱 vitamin B12
⚡ magnesium
🌊 algae-derived EPA/DHA
🌸 inositol in selected PMOS contexts
🧬 CoQ10
🌿 N-acetylcysteine
✨ targeted antioxidants or condition-specific nutrients
And yes, herbs may also have a place.
But not every hormonal woman needs Vitex, ashwagandha, maca and black cohosh all poured into one cup under a full moon. 😂
Sometimes she needs an herb.
Sometimes she needs food.
Sometimes she needs testing.
Sometimes she needs a prescription.
Sometimes she needs a referral.
That is personalised naturopathy.
Where to Buy Professional-Grade Supplements
🇺🇸 United States: Click here
🇬🇧 United Kingdom: Click here Code: KXCTGG
🔥 Temporary Elimination, Not Forever Restriction
A therapeutic elimination may be helpful when there is a clear reason.
The key words are:
Temporary. Structured. Reintroduced. Personalised.
Depending on the case, that may involve investigating specific symptom-provoking foods or using a short, structured approach for appropriate GI symptoms.
What I do not automatically remove from every hormonal woman is:
🚫 gluten
🚫 soy
🚫 legumes
🚫 grains
🚫 fruit
🚫 joy
That is not root-cause care.
That is dietary whack-a-mole.
🏋🏾♀️ Exercise for Resilience, Not Punishment
I love women building muscle.
But exercise is still a physiological stressor, so I look at:
Training + nourishment + sleep + recovery + health status
For some women, support may include:
🏋🏾♀️ resistance training
🚶🏾♀️ walking
🚴🏾♀️ enjoyable cardio
🤸🏾♀️ mobility and balance
😴 better recovery
For an under-fuelled woman, the answer may be:
Less output. More nourishment.
I am not interested in helping women become smaller, more exhausted and more hormonally miserable.
I want resilient women.
💗 Bioidentical Hormones Without the Fear or Marketing Fog
Bioidentical—or body-identical—hormones have a molecular structure identical to hormones produced by the human body.
Examples include:
🌹 17β-oestradiol
🌙 micronised progesterone
Appropriately prescribed hormone therapy can have an important place for selected women.
But this distinction matters:
Taking progesterone does not automatically mean you are ovulating.
Exogenous progesterone and ovulation are not the same physiological event.
My position is simple:
The right product, for the right woman, for the right reason.
Using hormone therapy does not mean you “failed naturally.”
Please release that guilt.
🧪 Test, Don’t Guess—But Test With a Question
Before ordering anything, I ask:
What question are we trying to answer?
Depending on the clinical picture, foundational evaluation may include:
pregnancy testing
full blood count
ferritin and iron studies
thyroid markers
prolactin
glucose and HbA1c
androgens
FSH, LH and oestradiol when appropriate
pelvic imaging
evaluation of abnormal bleeding
And please—can we stop testing every woman’s progesterone automatically on cycle day 21?
When serum progesterone is being used as evidence of recent ovulation, timing should relate to her actual cycle, often around one week before the expected next period rather than one universal calendar day.
Timing matters.
🏠 Mira: Bringing Ovulation Tracking Into Real Life
Not every useful piece of information has to come from one isolated blood draw.
For women wanting to understand hormone patterns across the cycle at home, I may consider Mira as a practical tracking tool.
Depending on the test wands used, Mira can track numerical urinary trends in:
🌹 E3G — an oestrogen metabolite that may rise as the fertile window approaches
⚡ LH — the surge associated with the body preparing to ovulate
🌙 PdG — a progesterone metabolite that may provide evidence of a post-ovulatory rise
🌱 FSH — available with selected options for additional cycle-pattern tracking
And here is the important distinction:
An LH surge is not the same thing as confirming that ovulation occurred.
LH tells us the body is signalling toward ovulation.
A subsequent PdG rise may add information about whether a post-ovulatory progesterone pattern followed.
That is why seeing the shape of the cycle over time can be useful for women with:
changing cycles
irregular cycles
suspected ovulatory variation
PMOS-type patterns
perimenopausal changes
But let me put my practitioner hat firmly back on:
Mira is a home monitoring tool—not a diagnosis in your handbag.
A Mira chart alone should not be used to diagnose PMOS, primary ovarian insufficiency, diminished ovarian reserve, infertility, perimenopause or luteal phase deficiency.
What it may offer is useful insight into:
ovulation patterns
cycle hormone dynamics
changes over time
especially when interpreted alongside symptoms, cycle history and appropriate medical testing.
The goal is not to obsess over every hormonal wiggle.
It is to learn your pattern and recognise when the data may be saying:
“Hmm… this deserves a closer look.”
🌿 Different Tools Answer Different Questions
Depending on the woman, I may consider:
🏠 Mira — home tracking of ovulation-related urinary hormone trends
🧪 DUTCH — selected hormone, metabolite, cycle-mapping and cortisol questions
🧬 DNAlife Hormones — genetic pathway context
🩸 FBCA — patterns and trends in conventional blood chemistry
💩 GI-MAP — when significant gastrointestinal symptoms justify stool assessment
🍓 MRT — in carefully selected, structured food-reactivity strategies
🩺 Conventional medical testing — because functional work should never replace appropriate medical investigation
Not automatically.
Not because more testing is always better.
But because:
Different tools answer different questions.
As a Traditional Naturopath and Functional Diagnostic Nutrition Practitioner, my role is to educate, identify patterns, use appropriate data, support nutrition and lifestyle foundations, look for healing opportunities, and refer or collaborate when needed.
That is what professional scope looks like.
🚨 Please Do Not “Balance Hormones” Around a Red Flag
Seek appropriate medical evaluation for concerns such as:
persistent loss of menstruation
possible pregnancy
very heavy or prolonged bleeding
bleeding between periods
bleeding after menopause
severe pelvic pain
fainting or marked dizziness
breathlessness with heavy bleeding
new headaches with visual changes
nipple discharge with cycle disruption
sudden major androgenic symptoms
major unexplained cycle changes
Please do not put castor oil on a red flag and call it root-cause medicine.
I say that with love. 🌿
🙏🏾 A New Season Is Not the End
Ovulation does not define your worth as a woman.
It is not the sole measure of health.
And less predictable ovulation during perimenopause is not evidence that your body has failed.
But ovulation is an important endocrine event.
Changes in ovulatory patterns may offer clues about:
🧠 brain-ovary communication
🌙 post-ovulatory progesterone patterns
🍽️ energy availability
🦋 thyroid and endocrine health
🎢 perimenopausal transition
🧩 wider Metabolic Chaos®
My faith shapes how I see the body.
“I am fearfully and wonderfully made.” — Psalm 139:14, KJV
That does not mean the body never experiences disease or dysfunction.
It means I approach it with respect.
Curiosity.
Stewardship.
And yes, my Seventh-day Adventist roots make me deeply appreciate the foundations:
☀️ sunlight
🌬️ fresh air
💧 water
🥗 nourishing food
🏋🏾♀️ movement
⚖️ temperance
🛏️ rest
🙏🏾 trust in God
Not as magical cures.
Not as tools to shame sick people.
But as part of wise stewardship.
Sometimes the healing opportunity is food.
Sometimes it is rest.
Sometimes it is a lab.
Sometimes it is a supplement.
Sometimes it is appropriately prescribed hormone therapy.
Sometimes it is a referral.
And sometimes it is simply recognising that your body has entered a new season—and deserves a new conversation.
🌳 Your Next Chapter Deserves More Than Guesswork
Perhaps you found this article because you are:
😰 hormonal
🎈 bloated
😴 exhausted
🧠 foggy
🔥 perimenopausal
🩸 dealing with changing cycles
🌙 waking at 3 a.m.
💼 trying to keep your professional life together while your body feels unpredictable
I see you.
And no, I am not going to promise that one herb, one test or one supplement will fix everything.
That is not how I work.
At Leaves from the Tree of Life LLC, we help Businesswomen who are Hormonal, Anxious, and Bloated through Functional Nutrition Coaching + Labs.
We look beyond:
“Take magnesium.”
We look beyond:
“It’s just stress.”
We look beyond:
“Your labs are normal.”
We investigate patterns.
We consider Metabolic Chaos®.
And most importantly?
We look for healing opportunities.
Depending on your individual needs, that may include:
🏠 Mira home hormone tracking
🧪 DUTCH testing
🧬 DNAlife Hormones
🩸 Functional Blood Chemistry Analysis
💩 GI-MAP
🍓 MRT
🥗 personalised functional nutrition coaching
🌿 naturopathic lifestyle support
🏋🏾♀️ movement and recovery strategies
🤝 appropriate collaboration and referral
Because this is not the end.
It may simply be time to learn the language of the woman you are becoming.
👉🏾 Click here to jump on a Discovery Call.
Invest in your health, invest in you, because a healthier lifestyle is a luxury you deserve!

🌅Golden Hour Harissa Lentil & Quinoa Stuffed Sweet Potatoes
with Lemon-Tahini Drizzle, Pomegranate Jewels & Pumpkin-Seed Crunch 🌿✨
This is the kind of meal I would pair with your ovulation beyond fertility blog because it quietly makes the point you keep returning to:
Sometimes the healing opportunity is not another supplement. Sometimes, ma’am… it is lunch. 😌🥄
Warm roasted sweet potato, savoury harissa-spiced lentils and quinoa, wilted greens, creamy lemon tahini, juicy pomegranate and crunchy pumpkin seeds. It is colourful, satisfying, whole-food plant-forward and substantial enough to feel like an actual meal—not three leaves arranged artistically around a chickpea. 😂
🌱 Whole-food plant-based
🥛 Dairy-free
🥚 Egg-free
🌾 Naturally gluten-free when all packaged ingredients are certified gluten-free
⏱️ Time
Prep: 15 minutes
Cook: 40 minutes
Total: approximately 55 minutes
Serves: 4
🛒 Organic Ingredients
🍠 For the roasted sweet potatoes
4 medium organic sweet potatoes
½ teaspoon ground cumin
½ teaspoon smoked paprika
Pinch of cayenne pepper or chilli flakes, optional
🌿 For the savoury lentil-quinoa filling
1½ cups cooked organic green or brown lentils
1 cup cooked organic quinoa
1 cup organic shelled edamame, cooked
1 organic red bell pepper, finely diced
2 packed cups organic baby spinach
2 cloves organic garlic, finely minced
1–2 teaspoons harissa paste, adjusted to taste
1 teaspoon ground cumin
½ teaspoon smoked paprika
2–3 tablespoons water or low-sodium vegetable broth for sautéing
Sea salt to taste, if appropriate for your needs
🍋 For the creamy lemon-tahini drizzle
¼ cup organic tahini
Juice of 1 large organic lemon
1 small organic garlic clove, finely grated
2–4 tablespoons water, to thin
Pinch of sea salt, optional
✨ For the gorgeous finish
½ cup organic pomegranate arils
¼ cup organic pumpkin seeds
½ cup chopped organic flat-leaf parsley
¼ cup chopped organic fresh mint
Extra lemon wedges
Chilli flakes, optional
👩🏾🍳 Step-by-Step Instructions
1️⃣ Roast the sweet potatoes 🍠
Preheat the oven to 200°C / 400°F.
Wash and dry the sweet potatoes, then pierce each one several times with a fork.
Place them on a lined baking tray and roast for approximately 35–45 minutes, depending on size, until completely tender through the centre.
You want them soft, caramelised and almost custardy inside.
2️⃣ Build the savoury filling 🌿
While the sweet potatoes roast, warm 2–3 tablespoons of water or vegetable broth in a large pan.
Add:
🧄 garlic
🫑 red bell pepper
🌶️ harissa
🌿 cumin
🔥 smoked paprika
✨ optional cayenne or chilli flakes
Cook gently for about 3–4 minutes.
Add the cooked lentils, quinoa and edamame. Stir well and heat for another 4–5 minutes.
Finally, fold in the baby spinach and cook just until wilted.
Taste and adjust the seasoning.
The filling should be savoury, smoky, slightly spicy and deeply satisfying.
3️⃣ Whisk the lemon-tahini drizzle 🍋
In a small bowl, combine:
tahini
fresh lemon juice
grated garlic
optional sea salt
Whisk.
The mixture may initially thicken—and yes, tahini enjoys being dramatic. 😂
Slowly add water, 1 tablespoon at a time, until the dressing becomes smooth, creamy and pourable.
4️⃣ Open the roasted sweet potatoes 🌅
Once tender, carefully slice each sweet potato lengthwise.
Gently fluff the centre with a fork.
Do not scoop everything out. We are making dinner, not excavating a building site. 😌
5️⃣ Load them generously 🥄
Spoon the warm lentil-quinoa filling into each sweet potato.
And I mean properly fill them.
This is not the moment for three decorative lentils.
6️⃣ Finish with the good stuff ✨
Drizzle generously with lemon tahini, then scatter over:
❤️ pomegranate arils
🎃 pumpkin seeds
🌿 parsley
🌱 mint
🌶️ optional chilli flakes
Serve with extra lemon wedges.
🌿 Health Benefits of Each Ingredient
A little practitioner note before we begin:
No single ingredient “balances hormones” or restores ovulation.
This meal is about creating a nutrient-dense, satisfying dietary pattern that provides fibre, plant protein, minerals, vitamins and phytochemicals. USDA FoodData Central is the main U.S. reference database for food composition, while NIH nutrient fact sheets provide evidence-based context for nutrient function and dietary sources.
🍠 Sweet Potatoes
Provide complex carbohydrate, potassium and carotenoid-rich plant pigments.
Why I like them here: They make the meal genuinely satisfying. For a woman who is under-fuelling, constantly restricting carbohydrates or training hard, adequate nourishment matters more than another “hormone hack.” Potatoes and many fruits and vegetables are recognised dietary sources of potassium.
🫘 Lentils
Provide plant protein, fibre, iron, magnesium and folate.
Why I like them here: Lentils bring both substance and nutritional density. NIH identifies legumes among dietary sources of magnesium and iron, while folate is essential for DNA synthesis and cell division.
🌾 Quinoa
Provides carbohydrate, protein, magnesium and other minerals.
Why I like it here: It helps turn the dish into a complete, substantial meal rather than a beautiful bowl that leaves you hunting for snacks 37 minutes later. Whole grains are among recognised dietary sources of magnesium.
🌱 Edamame
Provides plant protein and contributes minerals and other nutrients.
Why I like it here: It boosts the meal’s protein and texture while keeping the recipe plant-based. NIH lists soy products, beans, peas and lentils among foods that can contribute zinc to the diet.
And no, I do not automatically fear whole soy foods in every hormonal woman.
Context, ladies. Context. 😌
🫑 Red Bell Pepper
Provides vitamin C and colourful plant compounds.
Why I like it here: Beyond flavour and crunch, vitamin C can improve absorption of non-haem iron from plant foods—making the combination with lentils particularly thoughtful.
🥬 Baby Spinach
Provides folate and contributes magnesium and other micronutrients.
Why I like it here: Green leafy vegetables are recognised sources of magnesium, and folate supports DNA synthesis and normal cell division.
🎃 Pumpkin Seeds
Provide magnesium and other minerals, along with plant fats and protein.
Why I like them here: They add crunch while contributing to a meal built around food-first mineral intake. NIH specifically lists seeds among good dietary sources of magnesium.
🥄 Tahini
Made from sesame seeds and contributes plant fats, minerals and flavour.
Why I like it here: It makes the meal creamy and satisfying without dairy. Seeds are recognised contributors of magnesium, and nuts and seeds can also contribute other essential nutrients within a varied diet.
🍋 Lemon
Provides vitamin C and acidity.
Why I like it here: The acidity brightens the whole dish, while vitamin C is particularly useful in a meal containing plant sources of non-haem iron.
❤️ Pomegranate
Adds colourful plant compounds and fresh sweet-tart flavour.
Why I like it here: It makes the meal feel luxurious while adding variety from richly coloured plant foods. NIH describes colourful fruits, vegetables, legumes, herbs, nuts and seeds as sources of diverse phytochemicals.
🧄 Garlic
Provides flavour and naturally occurring plant compounds.
Why I like it here: It helps create depth without relying on excessive salt or bottled sauces. More importantly, delicious food improves the odds that a nourishing eating pattern is actually sustainable.
🌿 Parsley
Adds freshness and contributes micronutrients and plant compounds.
Why I like it here: Herbs are not merely garnish. They increase flavour complexity and plant diversity without turning the meal into a supplement protocol.
🌱 Mint
Adds cooling brightness.
Why I like it here: It balances the warm spices, rich tahini and sweet potato beautifully. Sometimes the health benefit of an ingredient is also that it makes the meal taste good enough to eat again.
🌶️ Harissa, Cumin, Smoked Paprika & Cayenne
Add heat, depth and aromatic flavour.
Why I like them here: They turn lentils from “responsible health food” into something you actually look forward to eating.
And that, quite frankly, matters. 😂
References
🌺 Ovulation, Menstrual Cycles & the Brain–Ovary Connection
ACOG. The Menstrual Cycle: Menstruation, Ovulation, and How Pregnancy Occurs.
https://www.acog.org/womens-health/infographics/the-menstrual-cycle [1]
Endotext / NCBI Bookshelf. The Normal Menstrual Cycle and the Control of Ovulation.
https://www.ncbi.nlm.nih.gov/books/NBK279054/ [2]
ASRM. Current Evaluation of Amenorrhea: A Committee Opinion.
https://www.asrm.org/practice-guidance/practice-committee-documents/current-evaluation-of-amenorrhea/ [3]
🌙 Progesterone, Neurosteroids & the Nervous System
StatPearls / NCBI Bookshelf. Physiology, Progesterone.
https://www.ncbi.nlm.nih.gov/books/NBK558960/ [4]
PMC / NIH. Allopregnanolone in Premenstrual Dysphoric Disorder: Dysregulation of the GABA-A Receptor.
https://pmc.ncbi.nlm.nih.gov/articles/PMC7231988/ [5]
PubMed. Efficacy of Micronized Progesterone for Sleep: A Systematic Review and Meta-analysis.
https://pubmed.ncbi.nlm.nih.gov/33245776/ [6]
🎢 Perimenopause, Changing Cycles & Hormone Therapy
NICE. Menopause: Identification and Management (NG23).
https://www.nice.org.uk/guidance/ng23 [7]
NHS. Menopause.
https://www.nhs.uk/conditions/menopause/ [8]
The Menopause Society. 2022 Hormone Therapy Position Statement.
https://menopause.org/wp-content/uploads/professional/nams-2022-hormone-therapy-position-statement.pdf [9]
The Menopause Society. Hormone Therapy.
https://menopause.org/patient-education/menopause-topics/hormone-therapy [10]
⚡ PMOS, Anovulation & Low Energy Availability
ASRM. PCOS Is Now PMOS: Understanding the Name Change.
https://www.asrm.org/news-and-events/asrm-news/latest-news/may-27-2026-pcos-is-now-pmos-understanding-the-name-change/ [11]
ASRM. 2023 International Evidence-Based Guideline for PMOS, formerly PCOS.
https://www.asrm.org/practice-guidance/practice-committee-documents/recommendations-from-the-2023-international-evidence-based-guideline-for-the-assessment-and-management-of-polyendocrine-metabolic-ovarian-syndrome-2023/ [12]
Endocrine Society. Functional Hypothalamic Amenorrhea Clinical Practice Guideline.
https://www.endocrine.org/clinical-practice-guidelines/hypothalamic-amenorrhea [13]
🌱 Nutrition, Deficiencies, Elimination & Exercise
NIH Office of Dietary Supplements. Iron: Fact Sheet for Health Professionals.
https://ods.od.nih.gov/factsheets/Iron-HealthProfessional/ [14]
NIH Office of Dietary Supplements. Vitamin B12: Fact Sheet for Health Professionals.
https://ods.od.nih.gov/factsheets/VitaminB12-HealthProfessional/ [15]
American College of Gastroenterology. Low-FODMAP Diet.
https://gi.org/topics/low-fodmap-diet/ [16]
World Health Organization. Physical Activity.
https://www.who.int/initiatives/behealthy/physical-activity [17]
🏠 Mira Home Hormone Tracking
Mira. Mira Hormone Monitor: Ultra4 Kit.
https://leavesfromthetreeoflife.fdnstores.com/mira-hormone-monitor-clarity-kit.html [18]
Bouchard TP. Using Quantitative Hormonal Fertility Monitors to Evaluate the Luteal Phase: Proof-of-Concept Case Study.
https://pmc.ncbi.nlm.nih.gov/articles/PMC9866173/ [19]
Pattnaik et al. Validation of Urinary Reproductive Hormone Measurements Using a Novel Quantitative Fertility Monitor.
https://pmc.ncbi.nlm.nih.gov/articles/PMC10247788/ [20]
🧪 Functional & Specialty Testing Tools
DUTCH / Precision Analytical. DUTCH Cycle Mapping.
https://dutchtest.com/cycle-mapping [21]
DNAlife. DNA Hormones.
https://www.dnalife.healthcare/products/dna/dna-hormones [22]
Diagnostic Solutions Laboratory. GI-MAP.
https://www.diagnosticsolutionslab.com/tests/gi-map [23]
Oxford Biomedical Technologies / LEAP. Mediator Release Test (MRT).
https://www.nowleap.com/the-patented-mediator-release-test/ [24]
🙏🏾 Faith-Aligned Whole-Person Health
Ellen G. White. The Ministry of Healing.
https://media4.egwwritings.org/pdf/en_MH.pdf [25]
Blog Disclaimer
The health information on this blog is for general educational purposes only and is not intended to diagnose, treat, cure, or prevent any disease. It should not be used as a substitute for professional medical advice. Always consult a qualified healthcare provider before making any health-related decisions
This blog may contain affiliate links, meaning Leaves from the Tree of Life LLC may earn a small commission if you purchase a product or service through these links—at no additional cost to you. Your support helps us continue to provide valuable content. Thank you!